"We describe a new clinical syndrome of primary new onset refractory status epilepticus (abbreviated NORSE).
Refractory Status Epilepticus (RSE) is a life threatening condition which is characterized by the failure to respond to first and second - line anticonvulsant therapy, i.e. benzodiazepines followed by phenytoin or fosphenytoin. Status epilepticus is "highly refractory" if the electrographic seizure activity is not terminated within 24 hours of achieving a burst suppression EEG pattern through continuous infusion therapy with propofol, pentobarbital or midazolam or a combination thereof."
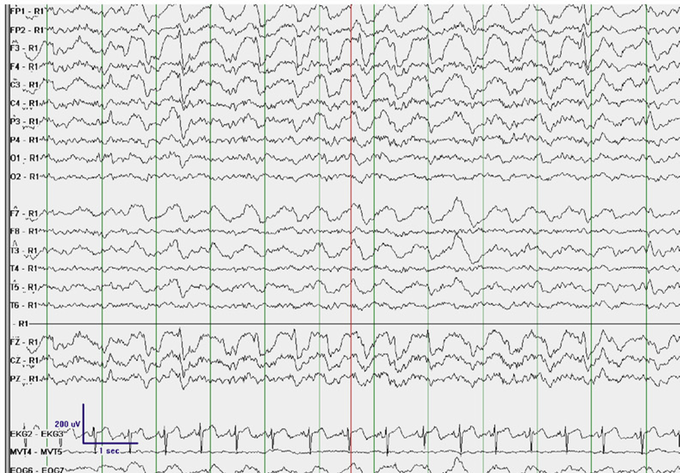
Panel shows electrographic seizure activity over the left frontal region (maximal amplitude at F3) on a referential montage with R1 placed over the 2nd cervical vertebra.
Epilepsy was classified as refractory when seizures did not respond or only partially responded to treatment with institution of two treatment regimens.
A common finding is lack of distinct features to suggest a viral etiology. "It is conceivable that the primary etiology in NORSE is in some instances immunogenic via a mechanism that remains to be discovered."
"Status epilepticus is a common and frequently devastating neurological emergency. In the vast majority of cases, a cause for status epilepticus is evident but in a small fraction of cases, the underlying etiology is not apparent despite extensive evaluation. Among these cases of cryptogenic status epilepticus, perhaps the most difficult to understand are patients who present de novo with highly refractory status epilepticus, which others have called NORSE."
Unifying features include female gender, young age, and catastrophic outcome. Unlike in other cases of resistant status epilepticus, extensive work-up including neuropathology did not reveal any underlying cause. Increased recognition of this clinical entity will help delineate its underlying etiology.
NORSE does occur in 10-20% of patients with etiologically proven infectious encephalitis, usually in the setting of a febrile illness, typically with meningismus and encephalopathy. In approximately 10% of cases of status epilepticus the cause is unclear, i.e. "cryptogenic". It is unusual not to discover an underlying cause for de novo status epilepticus, particularly when highly refractory, however, it does have typically devastating consequences.
Some common clinical features were young age of onset (average 28.5 yrs.), female preponderance, no prior history of seizures or neurological disorder and poor clinical outcome, (the abnormalities evident during this evaluation can be attributed to the ictal activity itself), either death or significant neurological impairment was the majority.
All cases seem to present with resistant status epilepticus, with no discernible cause and died within three months without abolition of seizure despite multiple medical interventions. Two patients which did not die survived in a vegetative state with frequent seizures.

Other duration of NORSE patients were 36 days in the hospital and long term morbidities were high. One patient died within nine days after receiving continuous infusion therapy with propofol, midazolam and pentobarbital. Propofol was the main-stay of infusion therapy. Post-mortem exam, a careful search was done but an infectious agent was not found. Consensus opinion of her caregivers was that she died due to the propofol infusion syndrome.